
Niger J Paed 2015; 42 (1): 9 –11
ORIGINAL
Ntia HU
Knowledge and attitude towards
Ekott M
sexually transmitted infections
Okwejie M
Nchewi A
among female students living in
Hagan M
hostels in a university community of
Afulukwe I
the south-south region of Nigeria
DOI:http://dx.doi.org/10.4314/njp.v42i1,3
Accepted: 14th August 2014
Abstract:
Introduction: A
cross
Igbo tribe 34%. Over 90% of the
sectional study was conducted in
subjects had heard of STIs. Vagi-
Ntia HU
(
)
the
female students’ hostel of the
nal itching (70.2%) and discharge
Ekott M, Okwejie M, Nchewi A
University of Calabar to deter-
(65.7%)
were
the
commonest
Hagan M, Afulukwe I
Department of Paediatrics,
mine their knowledge and attitude
symptoms reported. Despite the
University of Calabar Teaching
towards sexually transmitted in-
level of knowledge, some students
Hospital Calabar, Nigeria.
fections (STI).
still patronize Chemist 4.8% and
drhappinessntia@gmail.com
Methodology: A
structured ques-
self-injection administration 4.8%.
tionnaire was administered to
Conclusion: The
awareness of
STI
those who consented to the study.
is
high but the understanding of
Information obtained were age,
symptomatology is poor.
year of study, knowledge of
sexually transmitted infections.
Key words: Sexually
transmitted
Results: Most
subjects were
in the
infections, Female hostel, Tertiary
age
category
of
21-25years
Institution.
(56.2%) and predominantly of the
Introduction
Methodology
Sexually transmitted infections (STIs) constitute a huge
A
cross-sectional study using a self-administered ques-
health and economic burden for low income countries .
1,2
tionnaire was carried out in February 2012 among
World Health Organization (WHO) estimates that ap-
females university students resident in the hostels. The
proximately 340 million new cases of the four main
questionnaire was a structured one seeking age, religion,
curable STIs ( gonorrhea, chlamydia infection, syphilis
year of study, knowledge of STI, health seeking atti-
and trichomoniasis) occur every year, 75-85% of them
tudes. Every student in the female hostel was eligible to
occurring in developing countries . One in three sexu-
3,4
fill the questionnaire. The purpose of the study was
ally active females would have had an STI at least once
explained. Those who were willing to fill the question-
by
the age of 24years . Serious long term complications
5
naire were assembled in the students’ reading room
of
STI in women have been well-documented . There
3-5
where they were administered. The questionnaires were
are
misconceptions regarding STIs and therefore
distributed to intending participants in the hostel. Care
grossly underreported . The considerable social conse-
6
was taken to avoid influence from their peers. However,
quences attached to STI including stigmatization,
only four hundred and twenty questionnaires were com-
domestic abuse, abandonment as well as less likely to
pleted accurately. The information obtained was both on
receive appropriate and timely care .
3
knowledge and personal experiences of STIs. Data col-
In
low-income countries, STI often go undiagnosed and
lected was analysed using descriptive statistics and
untreated due to lack of knowledge. There is little
SPSS (v.18.0).
emphasis on education and other efforts to prevent STI
from occurring and therefore one of the reasons why STI
control programs often fail in low-income countries .
1
Understanding people’s knowledge regarding STI could
Results
provide an important basis for the development of inter-
ventions to promote early healthcare-seeking behavior
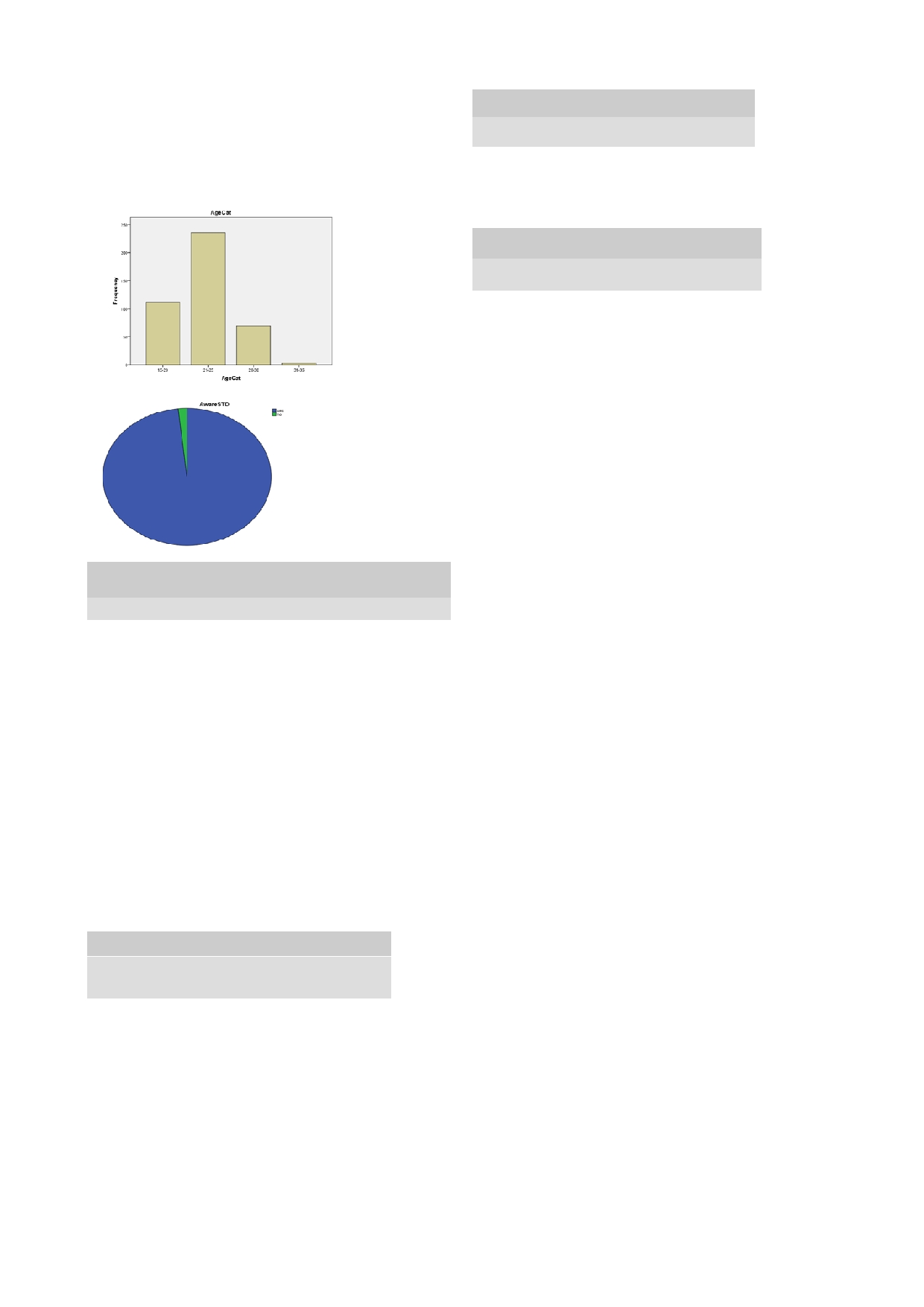
Most of the study population fell within the age range of
and protective practice for STI, as well as avoid its
21
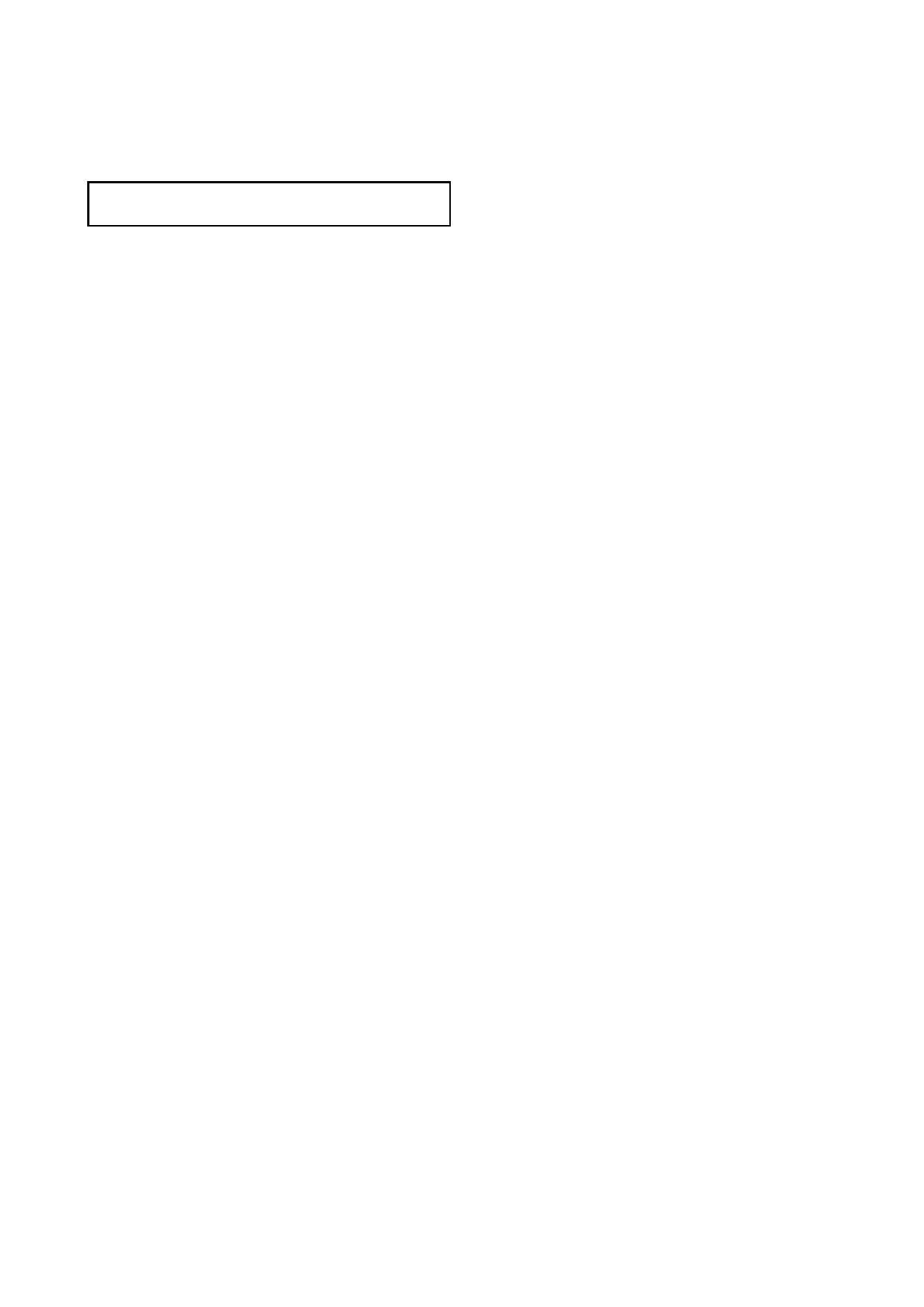
to 25 years (56.2%), Fig 1. Almost all the subjects
complications.
have heard of sexually transmitted infections (98.1%),
figure2. Christians dominated the study population
(98.8%) with of the Igbo tribe seen (34.0%), Table 1.
Vaginal itching was the frequently perceived symptom
10
(70.2%) followed by vaginal discharge (65.7%), Table
Table 3: Source
of information
2.
Bleeding and headache were least perceived. The
Source
Student
source of STI information was mostly from media
Yes
No
(55.7%), Table 3. Some female students (4.8%) still
Friend
151(36.0)
268(63.8)
patronize chemist for treatment of STI, Table 4.
Media
234(55.7)
185(44.0)
Lecture
200(47.6)
218(51.9)
Fig 1: Frequency
distribution of age
Table 4: Treatment
seeking behavior
categories
Treatment
Student
Yes
No
Enema
3(7)
416(99.0)
Sitzbath
39(9.3)
379(90.2)
Chemist
20(4.8)
399(95.0)
Injections
20(4.8)
399(95.5)
Doctor
396(94.3)
23(5.5)
Fig 2: STI
awareness
rate.
Discussion
In
this study we sought to establish the level of knowl-
edge
and attitude of STIs among female students resi-
dent
in female hostel in the University of Calabar. Of
the
420 students interviewed 98% had knowledge of
STIs. This study shows that higher level of education is
Table 1: Frequency
distribution of
socio-demographic
an
advantage on knowledge of STIs. A similar trend has
characteristics
been reported in other studies . Surprisingly, other au-
7,8
Variables
Percentages (%)
thors
9-11
found low knowledge of STIs among females
Age
15-20
26.7
studied. This difference may be attributed to religious
21-25
56.2
and
cultural beliefs were issues about sex education and
26-30
10.4
worse still sexually transmitted infections are kept in
31-35
0.7
secrets and hardly talked about in public. The study
Religion
Christian
98.8
population was predominantly Christians (98.8%) for
Muslim
0.7
the simple reason that this region is made of mostly
Others
0.5
Christians which may further explain why such a high
Tribe
level of awareness because this
religion encourages
Igbo
34.0
Ibibio
26.9
health education without limitations.
Efik
16.9
Others
22.1
The source of STI knowledge was mostly from media
Level of education
(55.7%). This may be due to the sensitive nature of the
100
20.0
200
29.5
issue, social stigma attached to it and feelings of shame
300
27.1
among students when talking about STIs.
400
15.8
Knowledge of the range of symptomatology of STI was
500
8.1
limited. Majority of the respondents knew of vaginal
itching (70.2%) and vaginal discharge (65.7%). Other
modes of presentation (fever, abdominal pain, bleeding,
Table 2: Knowledge
of symptoms
of STI
headache and body weakness) was limited. Most STIs
Symptoms
Presence of symptoms
may be symptomless coupled with the early onset of
Yes
No
sexual activities in adolescents which could make these
Fever
60(14.3)
359(85.5)
STIs go unnoticed with their consequent sequelae
5,9,12-14
.
Headache
32(7.2)
387(92.1)
Higher level of education and older age have been
Abdominal pain
113(26.9)
308(72.9)
reported to be associated with good health seeking
Vaginal itching
295(70.2)
122(29.0)
attitudes as reported by Vois in et al . We found a simi-
10
Vaginal discharge
276(65.7)
142(33.8)
Body weakness
65(15.5)
353(84.0)
lar trend in this study were over (94.3%) admitted going
Bleeding
32(7.6)
387(92.1)
to
see a medical Doctor.
Conclusion
The knowledge of STIs among the females in the
university community was high. However, knowledge of
11
the various ways of presentation of STIs was limited.
Acknowledgement
More
emphasis needs to be focused on the various mode
of
presentation in order to avoid some STIs from going
We
are thankful to the students in the hostel who despite
unnoticed.
their tight schedule made out time to respond to our
questions.
Conflict of interest: None
Funding: None
References
1.
Mayaud P, Mabey D. Approaches
10.
Voisin DR, Salazar LF, Crosby R,
20.
Sexually transmitted infection
to
the control of sexually transmit-
DiClemente RJ. Correlates of
general information. brown.edu/
ted
infections in developing coun-
sexually transmitted infections
studentservice/health_service/
tries: old problems and modern
prevention knowledge among Afri-
health_education/sexual_health/
challenges.
can
American girls. J
adolesc
sexually_transmitted_infections/
2.
Wilberforce KS, Jerome T, John
Health. 2012, 51: 197-9 .
ind.
CL,
Fred WM. Knowledge, atti-
11.
Hickey MT et al. sexually trans-
21.
Rukara KRM, Sekadde-Kiondu C,
tude and practice about sexually
mitted infection risk perception
Oyieke JB. J
Obstetr and
Gynecol
transmitted diseases among uni-
among female college students. J
East Central Africa 1995;11(1):
versity students in Kampala. Afr
of AmerAcad of NurPract. Ac-
19-22.
Health Sci 2001; 1(!): 16-22.
cessed July 2013.
22.
Miriam JT, Friday EO, Francesca
3.
World Health Organization
12.
Afolabi M, Darope V, Irinoye A,
OO,
Elisha PR, Paul C et al. Per-
(WHO). Global prevalence and
Adergoke A. (2013) Health-
ception of sexual behavior and
incidence of selected infections:
seeking behavior and student per-
knowledge about sexually trans-
overviews and estimates, WHO?
ception of health care services in a
mitted diseases among adolescents
HIV_AIDS/2001/02 Geneva:
university community in Nigeria.
in
Benin city, Nigeria. Interna-
WHO, 2001.
Health, J, 817-824.doi: 10.2436/
tional Family planning Perspec-
4.
WHO: Global Strategy for the
health.2013.55108.
tives, 1999; 25(4): 186-190 & 195
.
prevention and control of sexually
13.
Ward H, Mertens TE, Thomas C.
23.
Maria EC, lara ML, Jose AP, An-
transmitted infections: 2006-2015:
(1997) Health-seeking behavior
gela MDF, Maria DW, Paulo
breaking the chain of transmission:
and
control of sexually transmitted
CG.sexaul behavior and knowl-
who; 2007.
diseases. Health
policy plan.
edge of sexually transmittedinfec-
5.
Pham TL, Cecilia SL Ingrid
1997;12(1): 19-28.
tions among university students in
MNguyen TKC. Lack of knowl-
14.
Sexually transmitted infections
Sao
Paulo Brazil. Int
J Gynecol
edge about sexually transmitted
(STI) fact sheet. Women-
and Obstetr 2010. 110(1); 43-6.
infections among women in north
shealth.gov. (accessed July 2013).
24.
Voisin DR, Salazar LF, Crosby R,
rural Vietnam. BMC Infectious
15.
Mayaud P, Mabey D. Approaches
DiClemente RJ. Correlates of
Diseases 2009;9: 85.doi:
to
the control of sexually transmit-
sexually transmitted infections
10.1186/1471-2334-9-85.
ted
infections in developing coun-
prevention knowledge among Afri-
6.
Sexually transmitted infection
tries: old problems and modern
can
American girls. J
adolesc
general information. brown.edu/
challenges.
Health. 2012, 51: 197-9.
studentservice/health_service/
16.
Wilberforce KS, Jerome T, John
25.
Hickey MT et al. sexually trans-
health_education/sexual_health/
CL,
Fred WM. Knowledge, atti-
mitted infection risk perception
sexually_transmitted_infections/
tude and practice about sexually
among female college students . J
ind.
transmitted diseases among univer-
Amer Acad NurPract. Accessed
7.
Rukara KRM, Sekadde-Kiondu C,
sity students in Kampala. Afr
July 2013.
Oyieke JB. J
Obstetr and
Gynecol
Health Sci 2001; 1(!): 16-22 .
26.
Afolabi M, Darope V, Irinoye A,
East Central Africa 1995;11(1):
17.
World Health Organization
Adergoke A. (2013) Health-
19-22.
(WHO). Global prevalence and
seeking behavior and student per-
8.
Miriam JT, Friday EO, Francesca
incidence of selected infections:
ception of health care services in a
OO,
Elisha PR, Paul C et al. Per-
overviews and estimates, WHO?
university community in Nigeria.
ception of sexual behavior and
HIV_AIDS/2001/02 Geneva:
Health, J, 817-824.doi: 10.2436/
knowledge about sexually trans-
WHO, 2001.
health.2013.55108.
mitted diseases among adolescents
18.
WHO: Global Strategy for the
27. Ward
H, Mertens
TE, Thomas
C.
in
Benin city, Nigeria. Interna-
prevention and control of sexually
(1997) Health-seeking behavior
tional Family planning Perspec-
transmitted infections: 2006-2015:
and
control of sexually transmitted
tives, 1999; 25(4): 186-190 & 195.
breaking the chain of transmission:
diseases. Health
policy plan.
9.
Maria EC, lara ML, Jose AP, An-
who; 2007.
1997;12(1): 19-28.
gela MDF, Maria DW, Paulo
19.
Pham TL, Cecilia SL Ingrid
28.
Sexually transmitted infections
CG.sexaul behavior and knowl-
MNguyen TKC. Lack of knowl-
(STI) fact sheet. Women-
edge of sexually transmittedinfec-
edge about sexually transmitted
shealth.gov. (accessed July 2013).
tions among university students in
infections among women in north
Sao
Paulo Brazil. Int
J Gynecol
rural Vietnam. BMC Infectious
and Obstetr 2010. 110(1); 43-6.
Diseases 2009;9: 85.
doi:
10.1186/1471-2334-9-85.